
Nursing is a Universal Language?
- Mike
- Nov 6, 2022
- 4 min read
It has certainly been a minute since my last post, but so much has happened in a short amount of time. I’ve moved over 800 miles away to South Carolina: the furthest from home I have ever stayed for an extended period of time was Washington, D.C. Technically, D.C. is below the Mason-Dixon line, and life was certainly different compared to living in New England. Now I’m 500 miles further south, and realizing how different my personal and professional lives have become.
Nursing is a global profession with endless facets and changing variables. That being said, a nursing student only has to take one exam to practice in almost any state in the United States. Nursing in the United States requires students to take one specific exam called the NCLEX; this is the last obstacle standing in the way of an eager nursing student from achieving their goal of being a fully licensed medical professional. This exam allows for nurses to practice in all states in the United States so long as they are able to obtain a license to practice in each state.
Having passed my NCLEX exam, I assumed nursing practice and responsibilities would be nearly the same in every state. I was wrong.
Not saying that I would prefer to take a different exam for each state I practice medicine in, but the test is definitely not a “one size fits all” situation. There are a ton of similarities comparing where I came from to where I am now, but there seem to be more differences. People have the same chronic and acute conditions wherever you go but there seems to be an exponentially more chronically ill patient population down in the South than there is in the Northeast. The scope of practice for nurses is different and the expectations on the job are no longer the same.
Back home, hospitals hire RNs with associate degrees with the contingency that they will achieve their BSN within 2 years of working for the healthcare system. LPNs have essentially been phased out and nurses with Master's degrees are being pushed to get Doctorates. Nurses with Doctorates have the ability to: diagnose patients, prescribe medication, see new patients, and even open their own practices. Down here, it is a whole different ball game.
In the outpatient world down here, Medical assistants, LPNs, RNs, and BSNs essentially do all the same job; I do not know if this is because of the lack of staff, but the only difference seems to be the pay. My role has transitioned from helping save lives and working to creating lasting, positive change in the lives of patients to being a secretary for my assigned provider. I was hired as a Nurse to perform nurse-related duties, but have taken on the opposite role: scheduling appointments, facilitating surgeries, answering phones, dealing with angry patients electronically or on the phone or in person, preparing charts for clinic, stocking rooms, rooming patients, and babysitting patients who can’t bother to hold themselves accountable for their own health.
Everyday, I think to myself, “this is not what I signed up for.”
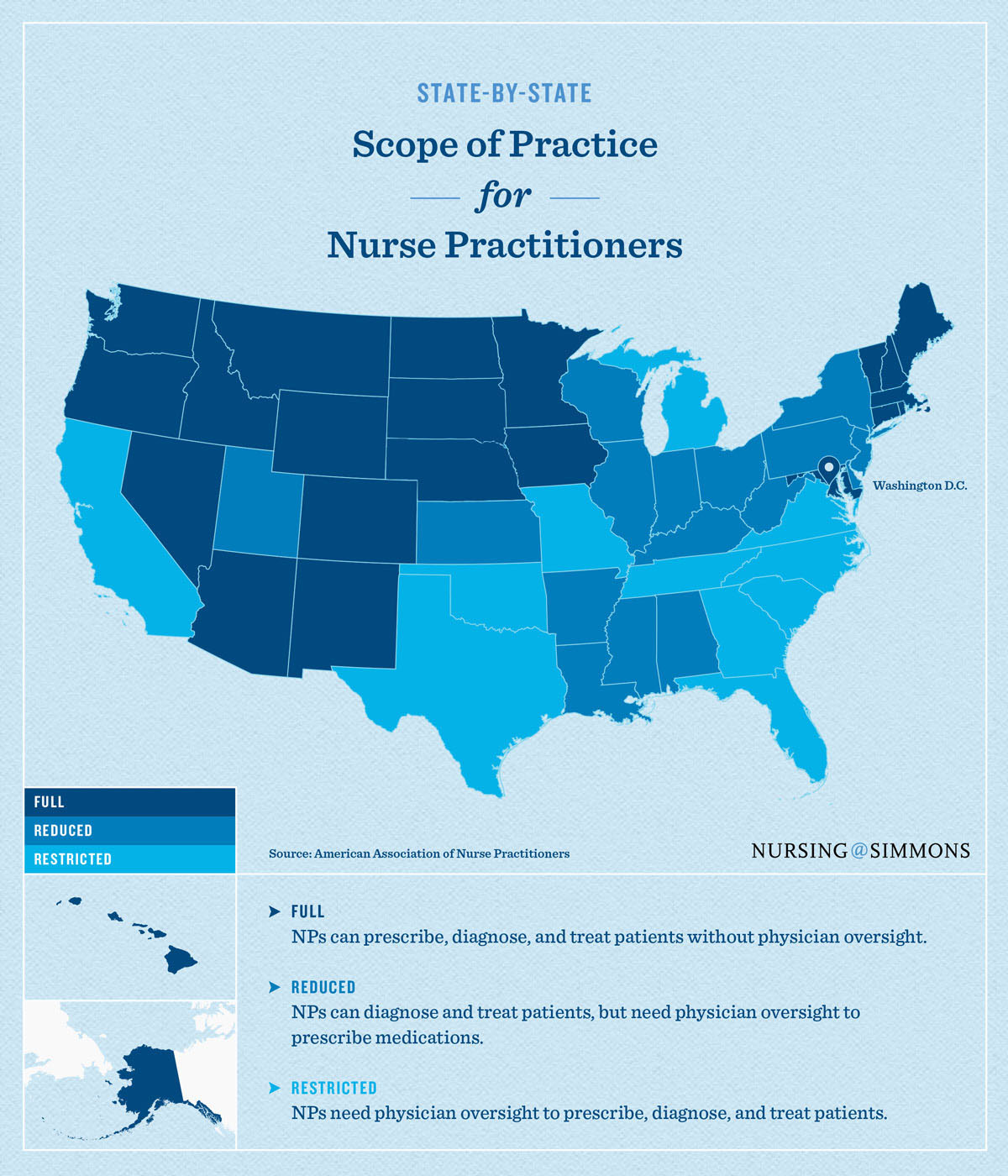
As someone who aspires to get their DNP, living in such a restrictive state is disheartening. The number of chronically ill patients is rapidly increasing and the number of providers is not. Patients are waiting almost a year for preliminary appointments, and critical illnesses cannot be given the time and attention they deserve. In fact, as of last Friday, our city's major hospital has a 2.5 day wait for a bed in the Emergency Department. Across the country, states are moving towards full autonomy of NP’s, whereas they can act with authority and without physician oversight. Those light blue states you see below, marked as restricted, they do not allow NP’s to act without written permission from a physician. If states are struggling to meet the needs of overwhelmed hospitals and desperate patients, why not ease that burden by expanding their provider network? Perhaps it is physician-centered organizations like the AMA petitioning against such measures. Perhaps another pandemic will cripple the healthcare system enough to create lasting change.
Yes, I do not have a real reason to complain about working in the outpatient world as I did this to myself. Working third shift in an understaffed setting in the middle of a pandemic destroyed every aspect of my life and transitioning to the outpatient setting is a way for me to reset for the next chapter of my life. Visiting the hospital, I spoke with many nursing staff, all of who warned me to stay away from the hospital setting as it is ruining all their lives; so as much as I complain about losing my vital nursing skills and the mundane routine, I made the correct decision. These days I may be moving at a sloth pace in outpatient healthcare, but angry patients cursing me out on the phone make me work up a sweat since nursing is my cardio.



Thanks for sharing such a nice blog keep it up.
MBBS From Armenia
MBBS From Micronesia
MBBS From Russia
MBBS From Belize
MBBS From Georgia
MBBS From Nepal
MBBS from Bosnia
MBBS From Bangladesh
MBBS From Kyrgyztan
MBBS Form Kazakhstan
GNM Nursing Course
BSc Nursing Course
Assistant Nursing Course